1 Farrer Park Station Road, #12-03, Farrer Park Medical Centre, Singapore 217562 (65) 6443 7713 
 There are 4 major ligaments in the knee. These consists of the anterior cruciate ligament (ACL), posterior cruciate ligament (PCL), medial collateral ligament (MCL) and lateral collateral ligament (LCL). There are also other ligamental structure to consider this includes the medial patellofemoral ligament as well as the structure in posterolateral corner and the posteromedial corner.
There are 4 major ligaments in the knee. These consists of the anterior cruciate ligament (ACL), posterior cruciate ligament (PCL), medial collateral ligament (MCL) and lateral collateral ligament (LCL). There are also other ligamental structure to consider this includes the medial patellofemoral ligament as well as the structure in posterolateral corner and the posteromedial corner.
Anterior cruciate ligament is to restraint any shifting of the tibial forwards (anterior displacement). It is also what it is termed as a secondary stabiliser and it reduces any varus valgus and any rotatory movement (side to side and turning movements i.e. instability). In patients with anterior cruciate ligament injuries this is often associated with sporting activities and sometimes can be from falls during activity such as running. In terms of the forces incurred it usually is associated with twisting injury and there is usually rotation and sudden hyperextension movements. Patients often describe a (pop) sound being heard and most times there is immediate swelling within a short period of time. In complete ACL tear they are usually unable to weight bear at the event.
Clinical examination will be to assess for instability using specific test such as Anterior drawer test and Lachman test. To quantify the ACL injury the assessment of instability is graded into 3grades. The most severe being grade 3 which is typified by more then 10mm of translation of the tibial against the femur. Xrays are useful to ruled out occult fractures and MRI is usually confirmatory of the ACL injury but is also useful in looking out for associated injuries such as collateral ligament and meniscal injury.
 Is anterior cruciate ligament essential to be reconstructed in all patients? There is continuous controversy in development of late arthritis in ACL deficient patients as compared to patients that have undergone ACL reconstruction. What has been established is that in patients with ACL deficient knee and associated meniscus tear these patients will do far better in reconstruction to reduce any further cartilage and meniscal injury. in patients who are very keen to return to sporting activities reconstruction of the anterior cruciate ligament provides stability and enables them to experience and improve the quality of life. If patients choose not to operate it is important for them to discuss on lifestyle changes to avoid repeated injury to the knee. Should they persist in continuing the sporting activities in the absence of the ACL it is highly likely they will incur in more injuries leading onto possible early osteoarthritis of the knee.
Is anterior cruciate ligament essential to be reconstructed in all patients? There is continuous controversy in development of late arthritis in ACL deficient patients as compared to patients that have undergone ACL reconstruction. What has been established is that in patients with ACL deficient knee and associated meniscus tear these patients will do far better in reconstruction to reduce any further cartilage and meniscal injury. in patients who are very keen to return to sporting activities reconstruction of the anterior cruciate ligament provides stability and enables them to experience and improve the quality of life. If patients choose not to operate it is important for them to discuss on lifestyle changes to avoid repeated injury to the knee. Should they persist in continuing the sporting activities in the absence of the ACL it is highly likely they will incur in more injuries leading onto possible early osteoarthritis of the knee.
 In patients who have partial tears with optimal physiotherapy it maybe possible to reduce the instability in the knee. However, the decision to return back high-level sporting activities has to be made in concert with the evaluation of the surgeon and the physiotherapist. In children who incurred in sporting injuries Dr Sathappan as done ACL reconstruction for as young as 14years of age. However, it is important to bear in mind the growth plate that is open in children surgical modification is very essential to prevent any physeal arrest in the children.
In patients who have partial tears with optimal physiotherapy it maybe possible to reduce the instability in the knee. However, the decision to return back high-level sporting activities has to be made in concert with the evaluation of the surgeon and the physiotherapist. In children who incurred in sporting injuries Dr Sathappan as done ACL reconstruction for as young as 14years of age. However, it is important to bear in mind the growth plate that is open in children surgical modification is very essential to prevent any physeal arrest in the children.
Conservative management in ACL injury involves reduction of swelling, improving the range of movement and physiotherapy. Physiotherapy involves a combination of static hamstring exercises with co-contraction of the hamstring and quadriceps muscles. As the patient regain hamstring and quadriceps control the therapist in the clinic will start to guide in proprioceptive training and bio feedback exercises. Thereafter, the patient will be put onto a specific protocol to allow certain amount of sporting activities to be regained by the patient.
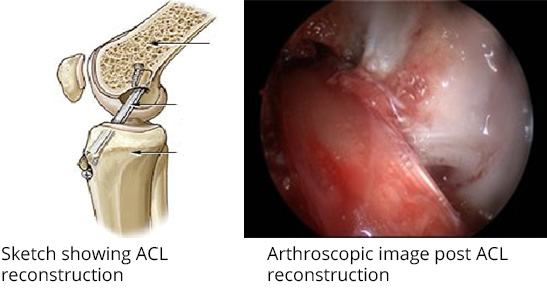
The surgical management of the anterior cruciate ligament involves the following aims:- i) restoration of joint anatomy; ii) provision of static and dynamic stability; iii) maintenance of the aerobic conditioning; iv) early return to work and sports. In ACL surgery most of the options for graft reconstructions involves either the usage of autograft (patient’s hamstring tendon) or allograft. Using specific ACL reconstruction guided systems optimal stability is attained by reconstruction the ACL ligament in the patient’s knee. It usually involves putting in of titanium based endobuttons and bio-degradable screws. When the graft is long and of optimal quality in selected patients they may not need any implants or any bio-degradable equipment to secure the graft into the knee joint.
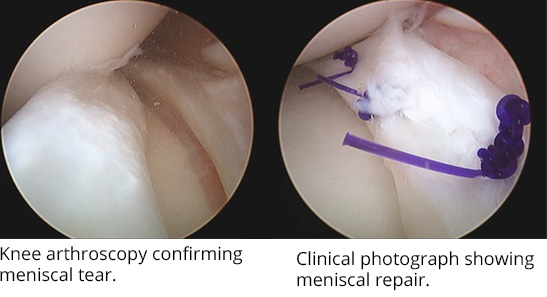
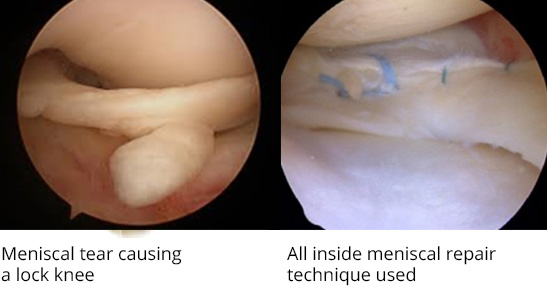 In this case example, there is a 46 year old carpenter who is a weekend regular soccer player. During the weekend game he heard a acute pop sound and tried to self-rehabilitate. He went back to soccer 2 months later. However, he incurred in acute twisting injury and the knee locked and was unable to walk, he presented to the clinic and had a MRI done. The MRI confirmed the patient who has initially incurred in ACL tear had went on to further injure the knee with a meniscal tear. Since he was unable to walk it was very essential for him to do a meniscal repair and ACL reconstruction. Following rehabilitation in clinic he was then sent to a sports therapist and with progressive therapy he recovered well and went back sporting activities and his occupation.
In this case example, there is a 46 year old carpenter who is a weekend regular soccer player. During the weekend game he heard a acute pop sound and tried to self-rehabilitate. He went back to soccer 2 months later. However, he incurred in acute twisting injury and the knee locked and was unable to walk, he presented to the clinic and had a MRI done. The MRI confirmed the patient who has initially incurred in ACL tear had went on to further injure the knee with a meniscal tear. Since he was unable to walk it was very essential for him to do a meniscal repair and ACL reconstruction. Following rehabilitation in clinic he was then sent to a sports therapist and with progressive therapy he recovered well and went back sporting activities and his occupation.