


PAINFUL CYSTIC SWELLINGS AROUND THE KNEE
Fibular lesions consisting of ganglions are not a common disease condition. In patients’ ganglions are often seen in the wrist and the foot regions. These are usually due to microtears in the capsule and the ligaments as well as the tendon sheath and can result in the seepage of fluid causing swellings in these regions. Less commonly, they can be also seen within bone.
Clinical case 1:
In this first patient who presented with painful swelling over the left knee region on the outer aspect (lateral). She was seen in the clinic for bilateral knee pain and has been having worsening pain in particular over the left knee. As part of a thorough assessment, it is important to localise the pain as being either in or around the knee. Unlike most patients, this is a lady who is 35 years old and it would be unusual for her to have joint line pain.
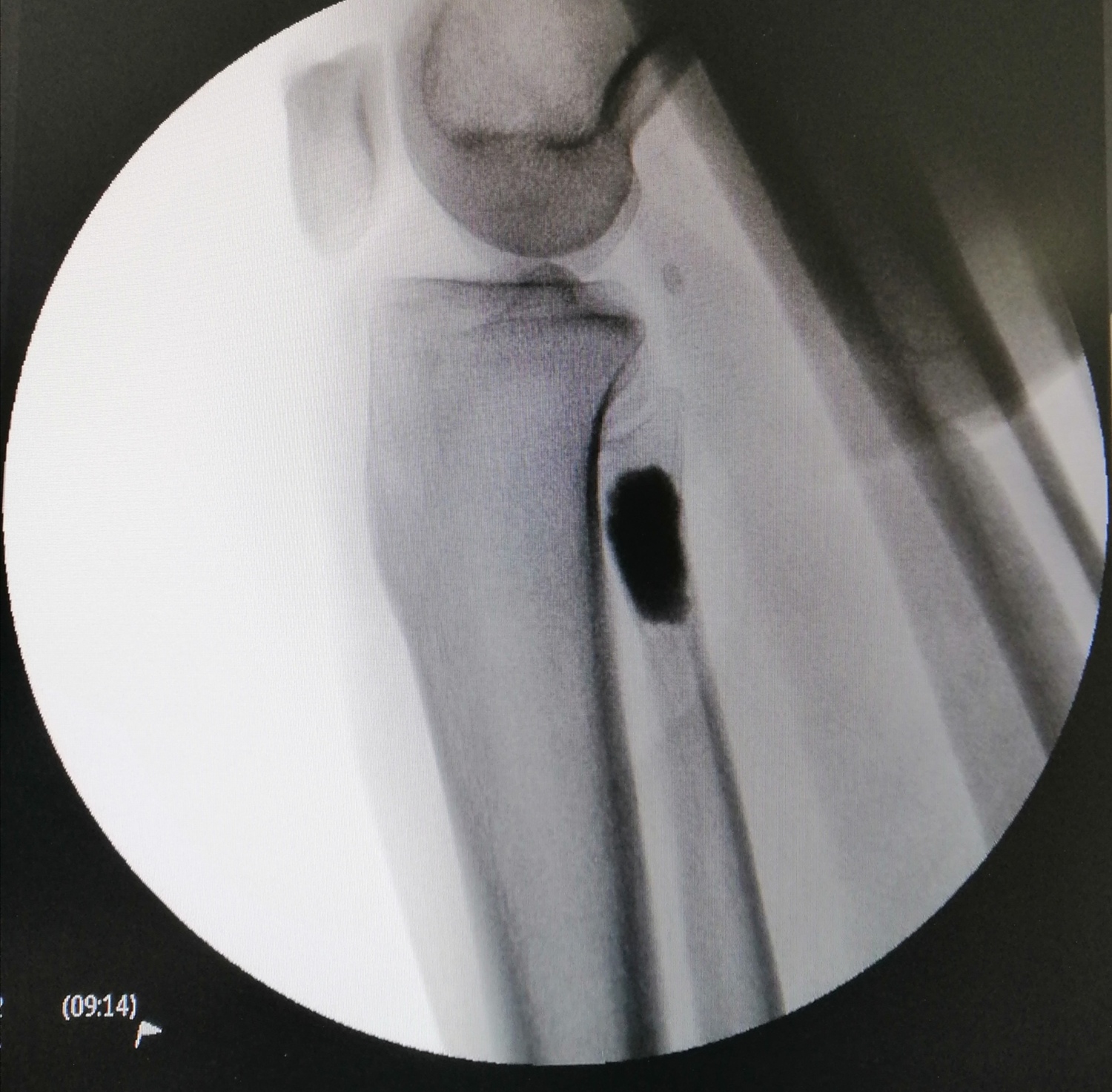
Further clinical assessment confirmed that the pain was localised to the fibula region. There was a noticeable swelling overlying the lateral border of the knee and associated with tenderness. In this patient, clinical assessment of the neurovascular status did not reveal any major abnormality. X-Rays were done as part of assessing her knee and confirmed no major joint line abnormality. However, there was a large cystic lesion in the fibula which raised the concern of possible soft tissue tumour. In view of these findings, she was advised for MRI.

MRI confirmed fibrous dysplasia appearance, which is a soft tissue tumour that can have the typical features of continual bony encroachment and enlargement. In severe cases, it can lead to compression of nerves. Fortunately, this was not seen in this patient. In view of her persistent symptoms, she was then advised for surgical intervention.

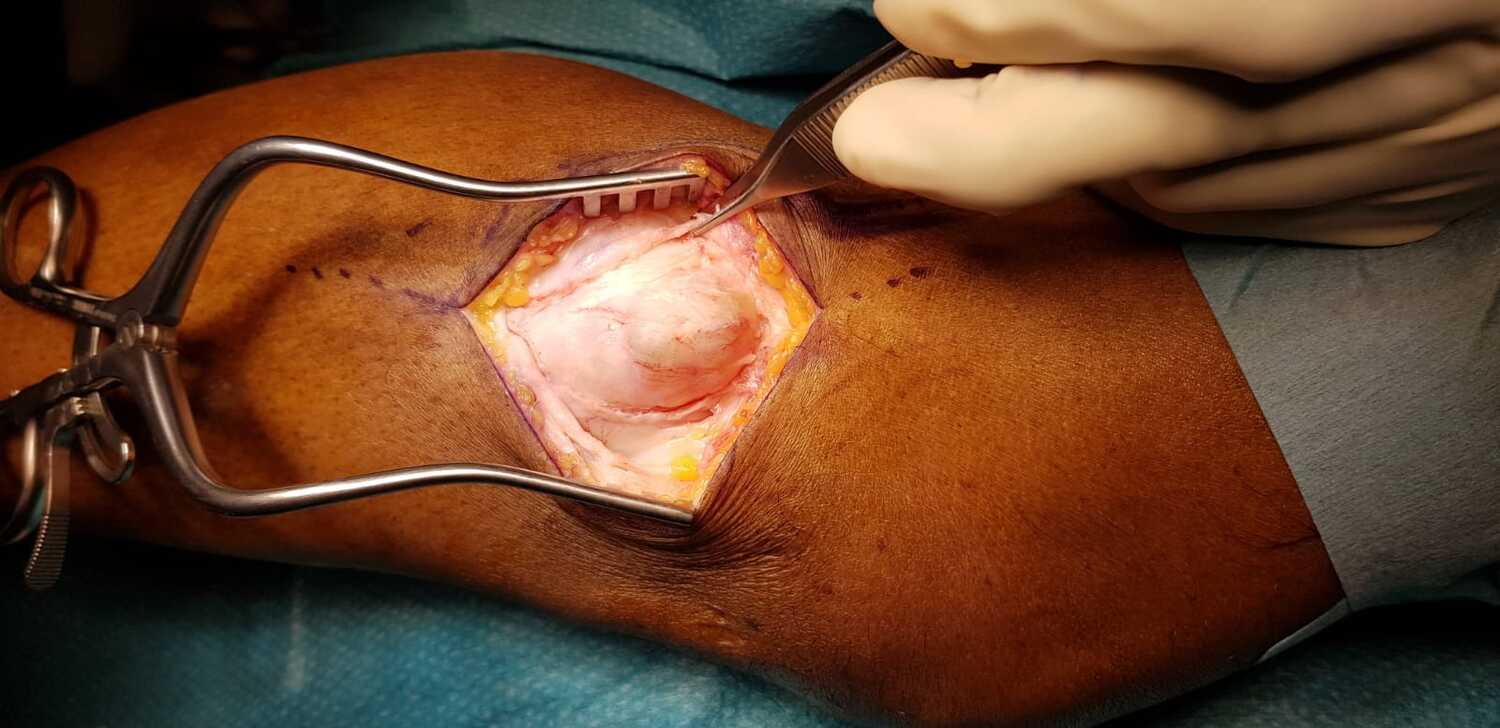
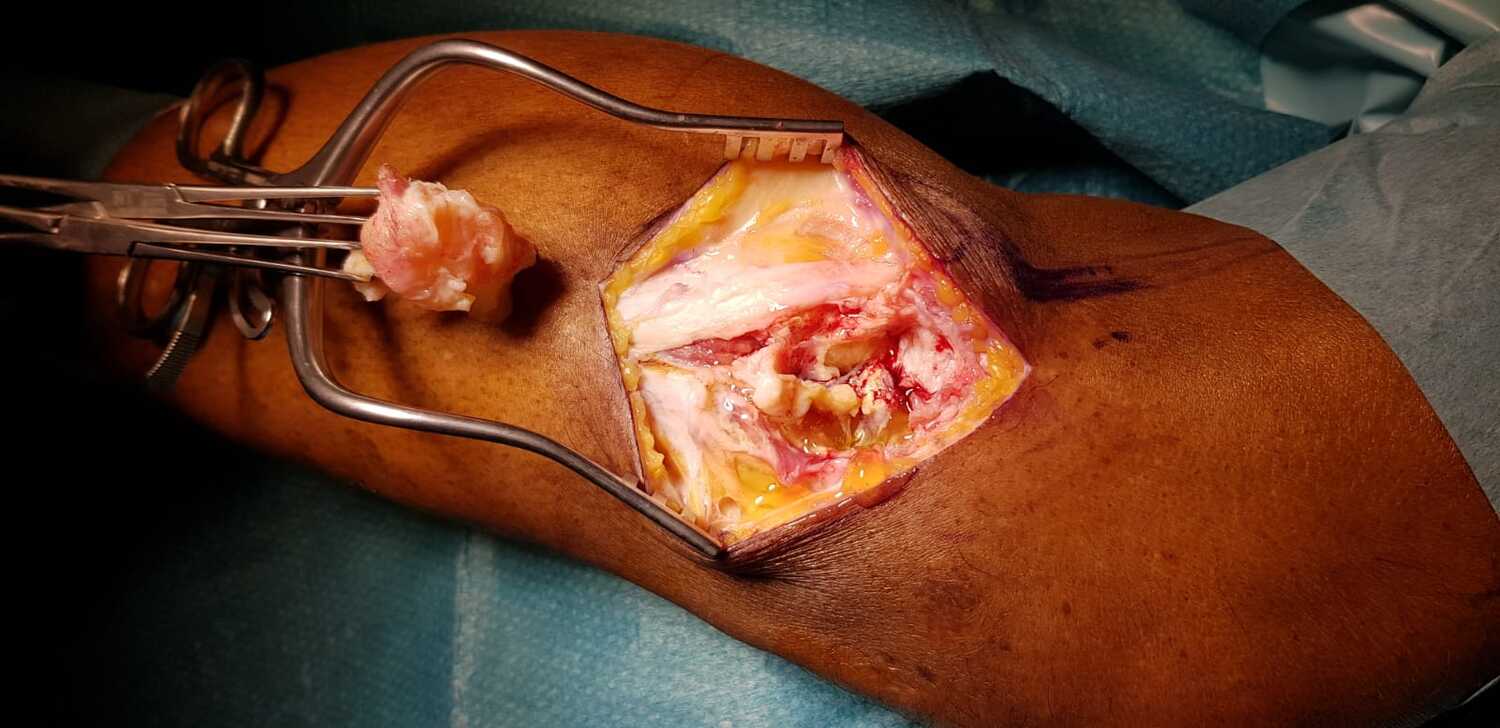
She underwent surgical intervention and at the time of surgery, there was noticeable, as per the clinical photographs a large cystic lesion with the encasement of soft tissue material that was gelatinous in nature. All the soft tissue materials were excavated and sent for histology which confirmed the benign nature of this lesion. Following clearance, there is always a natural void in the bone. This needs to be filled up to reduce the risk of recurrence as well as bleeding and some degree of heat-related treatment to kill off any microscopic cells that are remnant within the cyst. To address these situations, often bone cement is utilised. This was applied and the next photograph shows the clinical appearance of post-cement augmentation of this lesion.
She was then followed up in the outpatient setting with optimal recovery and X-Rays done at 2 years post-surgery show no recurrence of the lesion with optimal recovery. She has already been discharged from follow-up.
Clinical case 2:
A similar case such as this is shown in the other patient described below. In this patient, unfortunately, the cystic swelling was very large and produced both nerve compression and pain. The common peroneal nerve is a nerve that controls the upward movement of the foot. This nerve encircles the fibula next to the location where the lesion was seen on the X-Ray described below. The patient also has osteoarthritis of the knee but these are not affecting his functional status currently. In this patient, surgical intervention is paramount to prevent any further nerve compromise.
He also was advised for a similar procedure as the earlier patient. Importantly, in this patient, careful counselling has to be given regarding the likelihood of nerve injury. This is because of the proximity of the common peroneal nerve to the surgical site of procedure.
The clinical photographs taken intra-op do reveal the close proximity of the nerve and the cystic lesion. Following optimal surgical intervention, patient had symptomatic improvement in pain and over a course of 6 months to a year, there was also progressive nerve functional improvement.

Nerves that are compressed often take a period of anywhere between 6 months to 2 years for full recovery. Therefore, in this patient who showed progressive recovery, it is very suggestive of compressive neuropraxia which was due to the impingement effect of the cyst. Fortunately, he had early surgical intervention which gave an opportunity for nerve recovery.
Share this blog via: